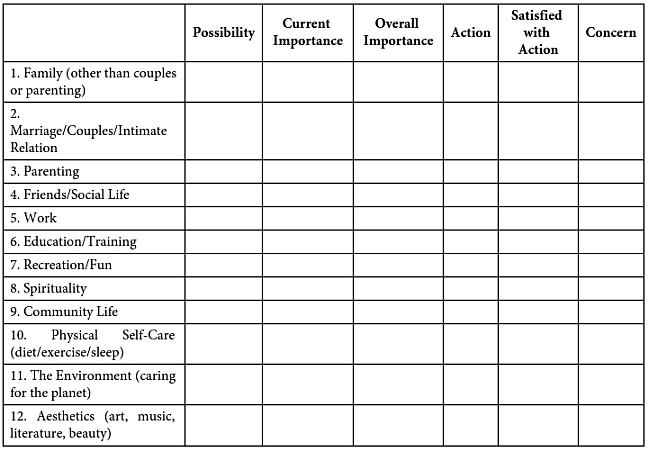
Below are areas of life that are valued by some people. We are concerned with your quality of life in each of these areas. There are several aspects that we ask you to rate. Ask yourself the following questions when you make ratings in each area. Not everyone will value all of these areas, or value all areas the same. Rate each area according to your own personal view.
Possibility: How possible is it that something very meaningful could happen in this area of your life? Rate how possible you think it is on a scale of 1–10. 1 means that it is not at all possible and 10 means that it is very possible.
Current Importance: How important is this area at this time in your life? Rate the importance on a scale of 1–10. 1 means the area is not at all important and 10 means that the area is very important.
Overall Importance: How important is this area as a whole? Rate the importance on a scale of 1–10. 1 means the area is not at all important and 10 means that the area is very important.
Action: How much have you acted in the service of this area during the past week? Rate your level of action on a scale of 1–10. 1 means you have not been active at all with this value and 10 means you have been very active with this value.
Satisfied with Level of Action: How satisfied are you with your level of action in this area during the past week? Rate your satisfaction with your level of action on a scale of 1–10. 1 means you are not at all satisfied and 10 means you are completely satisfied with your level of action in this area.
Concern: How concerned are you that this area will not progress as you want? Rate your level of concern on a scale of 1–10. 1 means that you are not at all concerned and 10 means that you are very concerned.
Addressing Pliance and Counterpliance
The therapist should also constantly assess other factors that may influence the client’s value statements, particularly those involving pliance and counterpliance. The therapist should be on the lookout for, among other indicators, the following signs that pliance or counterpliance might be influencing the process:
- Values statements controlled by the presence of the therapist, in conjunction with the client’s assumptions about what might please the therapist. Relevant consequences would be signs indicating the therapist’s approval and/or the absence of the therapist’s disapproval.
- Values statements controlled by the presence of the culture more generally. Relevant indicators would include the absence of cultural sanctions and broad social approval or widespread prestige.
- Values statements controlled by the stated or assumed values of the client’s parents. Relevant consequences would be parental approval—either actually recorded and/or verbally constructed.
- Values statements that have a “have to” quality that might indicate either fusion or avoidance.
- Values statements that are heavily laden with rumination about the past and/or worry about the future.
It is difficult to imagine a client who would have values that were not controlled in part or at times by all of these variables. The key question is whether removal of the relevant influence would significantly affect the potency of the value as a source of life direction. The task of assessment cannot be completed in only one discussion. The issue of “ownership” of the value is likely to resurface time and again. Some of these issues might be best addressed by asking the client to talk about the value while imagining the absence of a relevant social consequence.
To illustrate, consider a client who endorses the value of being well educated. The therapist might ask if the level of valuing (or the value itself) would change if it had to be enacted anonymously: “Imagine that you had the opportunity to further your education but you could not tell anyone about the degrees you had achieved. Would you still devote yourself to achieving it?” Or, “What if Mom and Dad would never know you pursued an education—would you still value it?” A different tack might also provide some insight into controlling variables. So, for instance, the therapist might ask: “What if you were to work very hard for a degree, and Mom and Dad knew and were proud, but the day after you received the degree you forgot everything you had learned. Would you still value it to the same extent?” As the client considers various imagined consequences, he or she may be chagrined to find that parental approval is the “straw that stirs the drink.” In this case, “becoming well educated” is not a value at all but rather a goal in the service of some other value (i.e., “being loved by and loving those who are in my life”). Once this value is clarified, it is written down as a desired end. It is not uncommon for some values to change in valence over the course of therapy or even as a function of the initial assessment.
The VLQ-2 asks the client to generate responses covering many separate life domains. Often, clients may come in with forms showing one or more domains left blank, or unresponded to. With more dysfunctional clients, all the domains’ response slots might be empty or might contain only very superficial answers. Here, the therapist needs to patiently discuss each domain in order to elicit responses from the client. Often, it helps to go back earlier in the client’s life and look for examples of dreams, wishes, or hopes that have disappeared because of negative life events. At other times, the therapist may have to assist the client either in identifying hidden values that underlie his or her specific life goals or, conversely, in generating specific goals based on well-described but ungrounded values.
It is not unusual for clients to list specific life goals that cannot be achieved. For example, a woman might say that she wanted to regain custody of a child she gave up for adoption 10 years earlier. In these instances, the therapist tries to find the underlying value and goals that might be achievable if one were moving in that direction. Another variation of this problem exists when the client focuses on unattainable life goals as evidence that irreparable damage has been done and yet there are no real meaningful life outcomes available in that domain. This latter possibility is more difficult to address clinically because values are now being employed in the service of the status quo, whereas the client’s perspective is that no change or only superficial change is possible. In such circumstances, it is often useful come into the present moment and have the client identify the specific feelings that appear in him or her whenever this sense of permanent loss is encountered. The therapist might ask the client to identify the value at the source of the pain (e.g., “I wanted to be a good mother and felt my meth addiction would eventually damage my child; that’s why I put her up for adoption”). Sometimes the source of the pain is a closely held value that the client followed at great personal cost. The therapist can help the client “connect” to the expression of this value without necessarily taking a pollyannaish stance on what has happened.